Building Member-Centered Research at Ascension Health
Creating shared understanding across one of the largest nonprofit health systems in the United States through behavioral archetypes, journey mapping, and strategic research that drove executive alignment on consumer experience priorities.

The Challenge
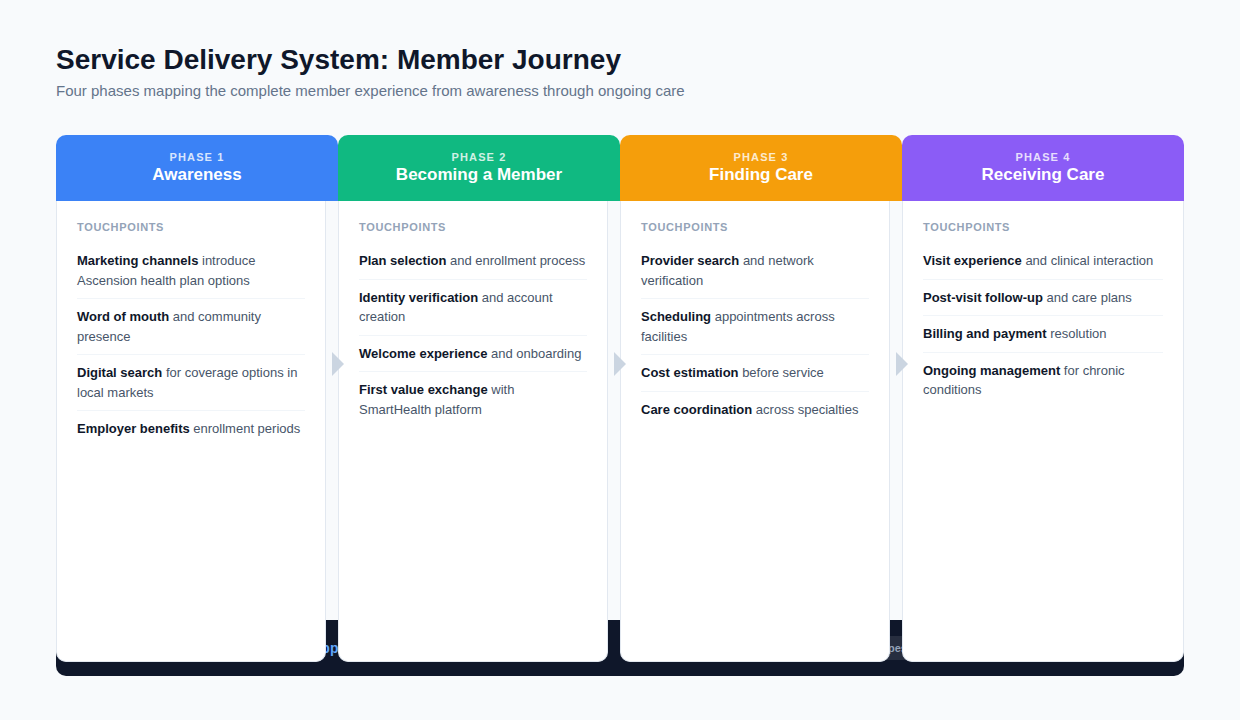
How do you create shared understanding across a large health system where internal employees, patients, and care teams all experience fragmented digital touchpoints?
Ascension is one of the largest nonprofit health systems in the United States. I joined as Senior UX Researcher, reporting to the VP of Digital and Consumer Experience Design, embedded in the consumer experience team working across internal and patient-facing digital initiatives.
Approach
Multiple digital transformation initiatives were underway simultaneously. I operated across parallel discovery and synthesis tracks, moving between immediate tactical research and longer-term strategic synthesis.
| Project | Methods | Deliverables |
|---|---|---|
| BigRocks Discovery | Open-ended response analysis, hand-coded thematic analysis | 3 primary themes (Network, Cost, Awareness), feature priorities for mobile team |
| SmartHealth Engagement | dScout diary study, behavioral archetype development | 3 archetypes, 5-stage engagement loop, engagement definition |
| Maternal Health Nudge Program | Qualitative phone interviews, SMS recruitment | Postpartum journey map, intervention timing recommendations |
| ACA End-to-End Experience | Phased usability testing, click-through prototypes | 4 rounds, 36 participants across 16 states, 5 direct design impacts |
| Identity Verification (IDDW) | Literature review, unmoderated study (dScout), Kruskal-Wallis | Trust perception findings, reversed recommendation, production design informed |

Key Findings
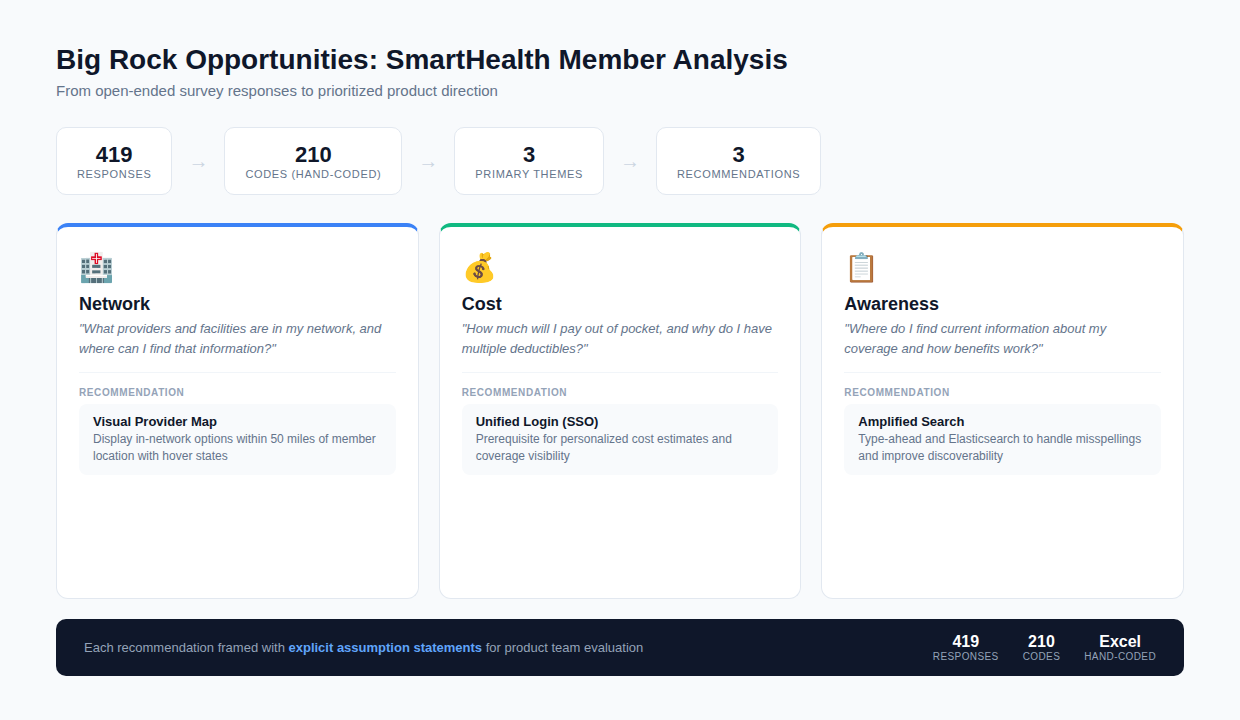
Analyzed 419 open-ended survey responses from SmartHealth member services feedback. Hand-coded 210 unique codes that bubbled up to three primary themes: Network (what providers are in my network), Cost (how much will I pay), and Awareness (where to find current coverage information). These became the reusable reference for subsequent SmartHealth research.
Three Behavioral Archetypes
Developed through a 7-part dScout diary study with 12 participants, structured around core values, health behaviors, and product engagement patterns:
- The Caregiver: Family-focused, others before self, quality directly tied to cost perception
- The Loyalist: Values-driven, seeks preventative services, avoids financial burdens
- The Truth Seeker: Evidence-based decisions, reactive to emergent needs, skeptical
Engagement Definition
The product team had no shared definition of engagement. I defined engagement as a multi-dimensional concept measuring frequency and duration of product use during a cycle of adoption, and developed a 5-stage engagement loop: Member Acquisition, First Session Value Exchange, Recurring Value Exchange, Trigger, Member Promotion. The framework gave the product team a lifecycle model for understanding when and why members engaged, and where the product was losing them.
Postpartum Intervention Windows Are Narrow
Maternal health research identified specific intervention windows where nudge-based outreach had highest engagement potential. Designed SMS-based recruitment using the same channel the program was already using, with a 15-day postpartum waiting period for ethical and clinical reasons. Qualitative feedback indicated patients felt cared for by the outreach.

IDDW Trust Perception Study
Literature consistently recommended disclosing third-party identity verification vendors to build user trust. A primary study reversed that recommendation: users trusted the experience more when the rationale was clear and the brand was familiar, regardless of vendor transparency.
Context
Identity verification had a 41% document verification failure rate, the single biggest source of drop-off in self-registration. The baseline pass rate was 59% against an 80% target. Every 1% improvement in pass rate translated to approximately 85 additional users completing registration.
Method
Started with a literature review on third-party trust perception in Customer Identity and Access Management (CIAM). Published research consistently recommended transparency: disclose the vendor, explain the process.
Then designed a primary study to validate before implementation. DScout express mission, unmoderated, n=36, 12 per condition, 3 conditions varying vendor disclosure and security messaging. Measured confidence, trust, and willingness to proceed. Chose Kruskal-Wallis as the non-parametric equivalent of ANOVA, appropriate for comparing three independent groups on ordinal measures.
Finding
Condition 2 (Ascension brand primary, security rationale provided, no vendor name) performed best: 47% preferred it. Confidence and trust scores were highest when the rationale was clear and the brand was familiar. The key mediating factor was whether the experience disclosed why verification was needed, which emerged during analysis.
A late constraint required the third-party vendor in the SMS URL. Went back to the research with the designer and determined to use strong security language and mention the third party by name in the SMS copy so it would not surprise users when they landed on a page with that branding.
Result
Leadership approved Option B. Research informed the production design even when constraints shifted mid-implementation. Through research and iterative design, the team reduced the failure rate by nearly half.
Key metrics: 41% baseline failure rate | 59% baseline pass rate | 80% target | n=36 | 3 conditions | Kruskal-Wallis | 47% preferred Option B | failure rate reduced by nearly half

ACA End-to-End Experience
Ascension launched an ACA insurance offering where six teams owned different parts of one customer journey. The post-enrollment experience had been tested with associates but never with ACA-eligible participants. Designed a four-round phased research strategy testing the end-to-end experience with real participants.
Method
Designed four phased studies across Summer 2021. Round 1 (May, n=9, web): post-enrollment with ACA members, looking for red flags. Round 2 (June): payment module. Round 3 (July, mobile): applying web learnings. Round 4 (August, web and mobile): full funnel. Each round iterated the prototype.
Collaborated with the designer to build a single click-through Figma prototype stitching together all six teams’ components. Coordinated with each team for latest designs. Tested with concurrent think-aloud protocol, 60-minute sessions.
Findings
Tax credit confusion led to disclosure redesign. HealthSherpa usage confusion led to clarified onboarding language. Payment ordering insight led to language changes. Dashboard feedback led to the “Hello, Diana” authenticated homebase. Autopay perception led to positioning it as a differentiator. Each finding tied directly to a design decision or action.
Result
36 total participants across 16 of 18 ministry states by end of summer. Three contributors to unified experience: (1) reducing uncertainty by explaining the process, (2) assessing whether order of operations confused customers, (3) encouraging account creation through value exchange explained earlier. When deployed, the team outperformed expectations on account creation.
Key metrics: 6 teams | 4 rounds | 36 participants | 16 of 18 states | 3 experience principles | 5 direct design impacts
Impact
Research Infrastructure Delivered
- Behavioral archetypes adopted across product teams as shared decision-making lens
- 5-stage engagement loop framework gave teams a lifecycle model for prioritization
- BigRocks themes became a reusable reference for subsequent SmartHealth research
- Postpartum journey research shaped nudge program intervention timing
- Mentored two junior researchers across concurrent studies, shaping methodology, reviewing outputs, and integrating findings into shared synthesis frameworks

Reflection
What Worked Well
- Archetype approach: Behavioral archetypes provided more actionable segmentation than demographic personas
- Working with existing data: The BigRocks analysis demonstrated that rigorous analysis of available data could produce actionable direction under time pressure
- Parallel tracks: Running discovery and synthesis simultaneously allowed quick wins while building longer-term strategic assets
What I Would Do Differently
- Connect internal and patient research earlier: The associate and patient experience parallel emerged late. Connecting these streams from the start would have strengthened both.
- Build archetype validation into quantitative work: Survey data confirmed archetypes but could have been designed to enable market sizing from the start